May 16, 2026 Charlie Sykes, who defined a life well lived, passed away at 92 years of age, on May 8. He is survived by his wife, Anya, two children who both pursued careers in international aid (his daughter, Agnieszka and Chris) and four grandchildren: Sasha, Coline, Lazlo, and Marek.
Anya Sykes wrote Charlie “lived a rich and meaningful life.”
Charlie spent 34 years with the private volunteer organization, CARE USA. After early postings in Greece (Field Representative) and Algeria (Deputy Director, 1961–63), he was Country Director successively for Poland, Pakistan, India, Egypt (1964–1980), and Dominican Republic (1978-1980).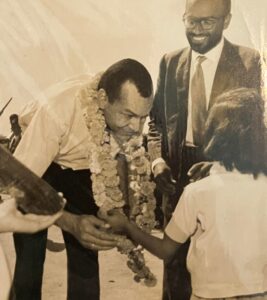
In the 1960s, Charlie took on one of the largest aid programs in the world, in India where CARE (then the largest aid agency in the world) managed feeding programs for children in schools. Dan Shaugnessy was with USAID in India at the time and remembers: “He directed some amazing and very successful CARE programs there that were jointly funded, including the huge CARE midday meals program, Project Poshak, the Balahar blended foods project, and other innovative programs.”
Colleague Franesca Nelson reflects: “Charlie’s unwavering commitment to nourish the hungry made perhaps the most significant contribution to the nutritional wellbeing of children in the twentieth century through CARE’s school feeding programs around the world. He was a visionary, …and most of all a wonderful human being.”
After his years managing large CARE programs in India and Pakistan, Charlie shifted to Washington, DC, working in close coordination with CARE’s President, Dr. Philip Johnston (who passed away three years ago). From 1980 to 1994 he served as CARE’s Vice President for Public Policy — the head of CARE’s Washington, DC office and its principal lobbyist on Capitol Hill. As Executive Vice President of CARE, Charlie was one of the most influential proponents of aid, shaping how Congress framed assistance legislation and appropriations. He was the lead voice among nonprofits in fighting for anti-hunger programs and food aid.
Former CARE Emergency Coordinator, Tom Alcedo writes: “Charlie always took the time to check with the field to ensure their position and interest were being considered, thus resulted in many positive outcomes, especially related to USAID and other USG funding. …During my time in Peru, Charlie was especially effective in getting our country office authorization to monetize excess farm commodities and program those funds to assist hundreds of thousands of people living in poverty. Charlie will be missed.”

Interviewed by management guru, Peter Drucker, Charlie explained: The most important thing in working with government is patience and cultural respect. Non-profits must be careful when working with other cultural groups. A leader must get to know an organization before collaborating with it
He collabrated closely with other NGOs in the Coalition for Food Aid.
Shaugnessy again: “He was a major proponent of NGO’s working with national and local governments and not trying to do things on their own. He believed NGO food aid could only be successful if it was carried out as a partnership with the host government, and he proved it with those successful programs. He carried that belief into later assignments including Egypt, Care New York, Care Washington, DC and finally as a Deputy Assistant Secretary of State in the 1990’s.”
Sykes was named a 1991 recipients of the Presidential End Hunger Award.
Ellen Levinson worked with him in the Coalition for Food Aid and remembers: “Driven by his knowledge of hunger’s devastating and generational impact, Charlie was instrumental in building a broad-based, national constituency for global food aid. He was both my mentor and a colleague, beloved for his warmth, insights, and dedication.”
After serving as Deputy Assistant Secretary of State, in the Refugee Bureau of the Department of State during the Bill Clinton presidency, which included travel to refugee camps in Africa, Charlie then accepted and served for over ten years from 2001-2011 – first as Treasurer, then Chair, and then as a regular Trustee of the international aid agency, Partners for Development (PFD).
Executive Director Jack Marrkand remembers: “Charlie had a deft touch in avoiding micro-management on operational matters but still ensuring that PfD was staying true to its mission and its overarching strategic plan. He was greatly respected by his colleagues on the board from whom he was able to elicit helpful input and advice.”
Fellow PFD board member and long-time friend, Wasiq Khan (sitting next to Charlie in the photo at right) remembers: “Charlie had this saint-like beatific quality to him. It was obvious when one was in his physical presence that he left his ego somewhere else and forgot to retrieve it. …. I think that quality of being above the fray, above self-dealing of any sort, was what gave Charlie the respect of his peers. It was the way Charlie listened patiently and always with profound empathy and genuine positive interest that drew so many of us to seek his counsel and company…. Wherever he went, he wanted to know where people were from, what their lives were like, how history had shaped their journeys. Charlie read voraciously and liked nothing more than chatting about a great book, a fascinating trip somewhere, or encounters he had had with interesting people. The world never ceased to fascinate. … he was a very free person. His mind could focus on the curious, the beautiful, the uncanny.”
listened patiently and always with profound empathy and genuine positive interest that drew so many of us to seek his counsel and company…. Wherever he went, he wanted to know where people were from, what their lives were like, how history had shaped their journeys. Charlie read voraciously and liked nothing more than chatting about a great book, a fascinating trip somewhere, or encounters he had had with interesting people. The world never ceased to fascinate. … he was a very free person. His mind could focus on the curious, the beautiful, the uncanny.”
Donna Ellis of PFD (shown with Charlie at right) says that he “was the kind of person who understood the balance between being a strong leader and remaining approachable. He was incredibly impactful holding a position of authority but still made a point to lead with warmth and a genuine smile.”
Armin Bušatlić, a Bosnian, ran the local Bosnia program implemented under Charlie’s tenure, and remembers how “dedicated he was in helping us handle the project crisis we faced; he clearly cared a lot about the work and did a lot of good for the region.”
PFD director William Graham recalls: “I am glad I had a chance to work with him. Charlie was easy going, well informed about the Bosnia program and I appreciated his guidance and feedback.” When Graham needed help getting his Macedonian wife immigration status, Charlie and his wife provided the critical support. “Tanja and I are forever grateful to Anya and Charlie for their support and guidance.” Charlie was proud of his wife Anya ‘s legal work, usually on behalf of immigrants , with AYUDA for many years.
Charlie was always an athlete, playing basketball and, until old age, tennis with his friends from the World Bank. One of them, Stephen O’brien, remembers: “On the tennis courts at the Arlington YMCA….was where he dominated! With his height and innate athletic ability he was virtually unbeatable by the rest of us. But we changed partners from set to set so at least once per match one could count on playing as Charlie’s partner and winning!
Jack Marrkand again: “Up until quite recently Charlie always stayed in touch with occasional calls and letters politely requesting updates about both work and family. At a lunch some years ago, Charlie gave me a copy of the book, “Black Ball Tales,” whose opening chapter profiles his father, Frank (Doc) Sykes.”
Charlie was deeply proud of his famous father, shown at right, one of the greatest American baseball pitchers of all time, who pitched 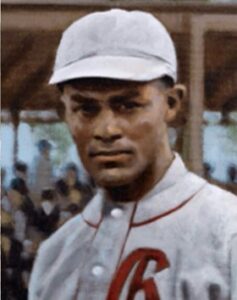 a no-hitter playing for the Baltimore Black Sox, with a career 3.5 ERA over 15 competitive seasons.
a no-hitter playing for the Baltimore Black Sox, with a career 3.5 ERA over 15 competitive seasons.
Known as “Doc Sykes” he challenged the segregationist policies of the time. He fought for the integration of juries nationally beginning with the Scottsborro trial in Alabama where he testified for the nine young African-American boys in 1931 facing an all-white jury. Considered seminal in the advancement of U.S. judicial equality, the Scottsboro trials were held after two white women, falsely accused nine boys, ages 12 to 20, of rape in order to justify their own whereabouts illegally onboard an interstate cargo train. Doc Sykes’ testimony along with the whole trial experience later influenced novelist Harper Lee when she wrote To Kill a Mockingbird, a best-seller, and which was rendered into one of the most important movies of all time, and won 8 Academy Awards including “best picture” in 1963.
In the Scottsboro trials, the accused’s collective guilt was pre-judged by the public, with newspaper headlines assuming their responsibility before all-white juries tried, convicted and sentenced to death all but one defendant in a matter of a day. Doc (in fact he was a dentist) Sykes testified about the qualifications of Black residents to serve on juries, presenting a list of around 200 qualified Black potential jurors in the area. In doing so he challenged the systematic exclusion of Black citizens from jury pools (and thus the all-white juries), which violated fair trial rights. His testimony helped highlight pervasive racial discrimination in jury selection. Very soon thereafter, the U.S. Supreme Court ruled (e.g., Powell v. Alabama in 1932 and Norris v. Alabama in 1935) that defendants were entitled to fair jury selection processes, advancing equal protection under the law.
The Scotssboro cases exposed the deep-seated racial biases of the Southern legal system to the world. Seeing how the machinery of justice could be entirely subverted by racial prejudice left a permanent impression on novelist Lee. When she set out to write her masterpiece in the late 1950s, the Scottsboro trials served as her historical blueprint for the systemic injustice she wanted to critique in To Kill a Mockingbird.
The model of Doc Sykes standing up for racial justice influenced Charlie to fight for humanitarian themes around the world, a life of service in and out of government. During his years with CARE, the nonprofit distributed some 12 million metric tons of food aid to some 150 million people, mostly children.
Jack Marrkand again: “It was a privilege to know Charlie Sykes for many years and to be guided and inspired by his commitment, unfailing optimism, and wisdom.”
Wasiq Khan, again, sums up the views of many, “We were drawn to Charlie because we wanted to be just a little bit more like him: handsome and athletic into his eighties, great conversation on almost any topic, and the feeling that you were heard and understood by someone you trusted deeply.”





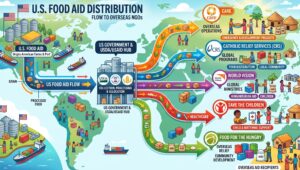 intense competition for these new FFP program awards is expected. NGOs such as CARE, CRS, World Vision, Mercy Corps, Save the Children and Action Against Hunger are expected to be seeking FFP grants.
intense competition for these new FFP program awards is expected. NGOs such as CARE, CRS, World Vision, Mercy Corps, Save the Children and Action Against Hunger are expected to be seeking FFP grants.
 communities in need.
communities in need.

 Diseases Hospital in Dhaka admitted 560 suspected measles cases in the first three months of 2026, compared to just 69 cases in all of 2025. (
Diseases Hospital in Dhaka admitted 560 suspected measles cases in the first three months of 2026, compared to just 69 cases in all of 2025. (
 would later become UNHCR), where he continued to use his fame as a polar explorer and diplomat to call attention to the victims of famine and genocide in Russia, Ukraine, and Armenia. In 1922, Nansen received the Nobel Peace Prize for his tireless work for refugees in Europe after the war.
would later become UNHCR), where he continued to use his fame as a polar explorer and diplomat to call attention to the victims of famine and genocide in Russia, Ukraine, and Armenia. In 1922, Nansen received the Nobel Peace Prize for his tireless work for refugees in Europe after the war.
 remain siloed within organizational systems and responsibilities, weakening crisis response.
remain siloed within organizational systems and responsibilities, weakening crisis response.


 they’re able to invest in the business. And so we see better impacts — both in terms of increasing income, savings, and nutrition….We’ve been rolling out a program called DreamSave, which is a digital bookkeeping application at the savings group level that runs on a smartphone. That’s been really well received and has had some positive impacts on the actual savings of the savings groups.”
they’re able to invest in the business. And so we see better impacts — both in terms of increasing income, savings, and nutrition….We’ve been rolling out a program called DreamSave, which is a digital bookkeeping application at the savings group level that runs on a smartphone. That’s been really well received and has had some positive impacts on the actual savings of the savings groups.”


 – the Struggle For Food and Dignity in Recent Humanitarian Crises” was a 2007-08 Hunger Watch Report by Action Against Hunger. It
– the Struggle For Food and Dignity in Recent Humanitarian Crises” was a 2007-08 Hunger Watch Report by Action Against Hunger. It