



May 21, 2026 The new study, Health in a World of Crises and Impunity, by the Johns Hopkins – Lancet Commission about Health, Conflict & Forced Displacement, was published this week in the Lancet Journal, with two dozen main authors (commission members), led by Dr. Paul Spiegel. It critiques the current ways that humanitarian aid flows as “unfit for purpose” because it relies on politicized funding models that ration survival rather than saving lives.
The “Johns Hopkins Center for Humanitarian Health-Lancet Commission” worked for almost three years in leading up to the publication on May 19, 2026 on the Lancet journal’s website, accompanied this week by a launch event in Geneva. The Commission comprises 42 authors from 20 countries, nearly all academics from universities, some with prior field experience. It includes no representatives from private industry, governments, digital health or technology companies, the military, or financial institutions.
Their 76-page report also notes “Conflict disrupts food production, markets, livelihoods, and humanitarian access, undermining household coping mechanisms and leading to acute and chronic undernutrition among displaced populations and host communities alike.” Hunger follows from economic harms and job loss: “Most conflict-affected populations have unstable or no income, affecting 78% of IDPs in Afghanistan and 70% in Iraq in 2022. In Sudan, unemployment in urban households increased by more than ten-fold after the conflict began.” For example, refugees often lack access to legal employment in countries of asylum.
While the study addresses food and nutrition, it does so only to a limited degree, placing hunger and malnutrition within a broader public health context. In its historical review, it highlights high malnutrition rates in Sudan, Yemen, and the Democratic Republic of the Congo (DRC). The report notes: “Undernutrition is a central pathway through which conflict increases mortality, contributing to more than half of infectious disease deaths globally in children.” Malnutrition significantly raises the likelihood of dying from communicable diseases such as malaria or measles.
Poor nutritional status, the Commission finds, “weakens immune responses, reduces vaccine effectiveness, and prolongs recovery from infection and injury.” It adds: “Recurrent displacement and prolonged food insecurity contribute to wasting, stunting, and micronutrient deficiencies, with long-term consequences for physical growth, cognitive development, and future health.”
The Commission report has many recommendations about reforming the aid system overall, but few that are specifically about food systems, resilience, agriculture, supply chains of recovery foods (such as RUTF), food fortification, school feeding, or other anti-famine programs. The report largely ignores food aid except to criticize its availability in Gaza, and to diminish it in comparison with cash hand-outs, though the report notes the World Food Programme’s large role in humanitarian aid.
In an accompanying editorial in the same issue of the Lancet (shown above), the editors summarize the findings, including a call to “invert power by shifting resources and decision making to affected populations, making external leadership exceptional, and strengthening nationally led health and social protection![]() systems.” And then concludes: “Creating an effective community-centred humanitarian system that provides a more just, robust, and sustainable future needs to be managed carefully and responsibly. “
systems.” And then concludes: “Creating an effective community-centred humanitarian system that provides a more just, robust, and sustainable future needs to be managed carefully and responsibly. “
The Commission names climate as both driver and amplifier:
- * Droughts, dust storms, and floods drive food insecurity, resource competition, and erosion of coping strategies in Somalia, South Sudan, Afghanistan, and the Sahel
- * Climate impacts “interact with pre-existing political, economic, and social vulnerabilities, pushing fragile contexts beyond critical thresholds”
- * Women particularly affected where they “have limited access to material, social, and institutional resources to cope with, absorb, and recover from climate-related shocks”
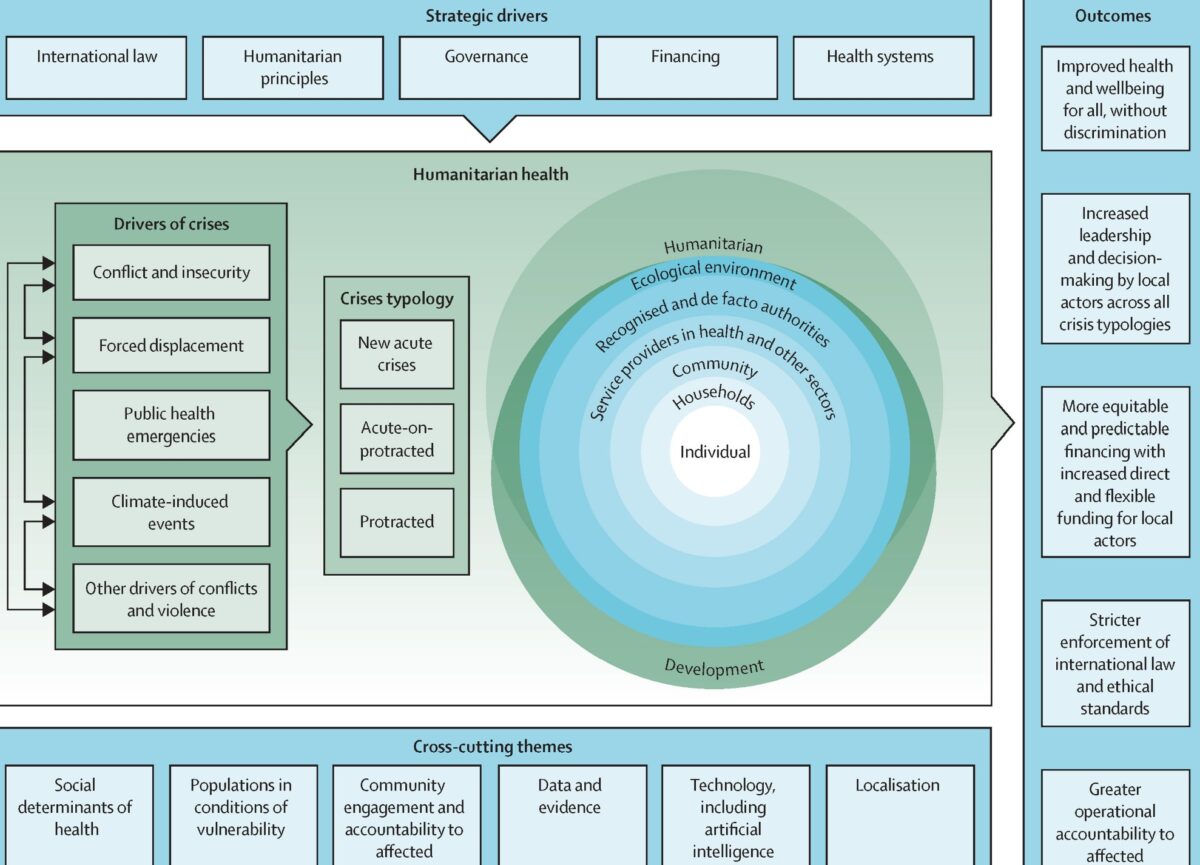
Most of the report talks at a higher level. A key finding and recommendation: “Humanitarian health action remains overly focused on short-term service delivery rather than sustaining health systems across crisis cycles. Fragmentation, disrupted financing, workforce losses, weak integration, and weak digital foundations undermine continuity, quality, and resilience, especially in protracted crises. Emerging technologies and artificial intelligence offer important opportunities to improve early warning, triage, supply chains, clinical decision support, and system planning, but without equitable access, regulation, and accountability they may also deepen exclusion and risk. The way forward is to prioritise health systems protection, ensure continuity and quality of care, integrate humanitarian and national systems where feasible, and invest in preparedness, workforce capacity, climate-resilient services, and ethically governed digital and artificial intelligence capacities that support more resilient, adaptive, and accountable health systems.”
Many readers of the report were pleased to see a vision for a “humanitarian reset.”
The authors try to be bold and do not shy away from controversy. For example, they call for one big UN agency for humanitarian aid, not the many independent agencies with distinctive mandates seen now. Repeatedly the report refers to “global health governance and “humanitarian architecture” as if there is now one coordinated system in place that is ill-conceived, as opposed to an ecosystem of independent actors each pushing progress in distinct ways. While acknowledging the history of humanitarian aid, and in particular groups like UNHCR, World Heath Organization, and the Red Cross, it gives little attention to the thousands of initiatives pioneered by individuals or independent nonprofit or voluntary organizations, directly helping communities in need.
communities in need.
The Commission lumps a lot of “humanitarian” assistance into one concept but does not discriminate between natural disasters and conflict-related crises. The authors argue that all aid should conform to national policies, even if the government in question are at war with groups of their own citizens.
The report’s strong push for massively expanded multipurpose cash assistance does not address funding sources or potential trade-offs with service provision, vaccination campaigns, food aid to fight famine, shelter materials, etc.
Some readers found the tone strident. For example the word “must” appears 86 times, giving the impression that the authors are issuing commands without specifying to whom they are directed.
Other launch events are scheduled in other cities.
Supplementary appendix includes
The New Humanitarian reviews the report here.
Numerous podcasts feature the study. Johns Hopkins’ 20 minute podcast about this can be found here.

 Diseases Hospital in Dhaka admitted 560 suspected measles cases in the first three months of 2026, compared to just 69 cases in all of 2025. (
Diseases Hospital in Dhaka admitted 560 suspected measles cases in the first three months of 2026, compared to just 69 cases in all of 2025. (