



June 6, 2026. Dr. Gary Slutkin, in his new book The End of Violence (published April 21, 2026), explains his early career experience working with the Somali Refugee Health Unit, helping malnourished refugees in East Africa, which inspired him in time to apply the skills he learned to take on global outbreaks of violence, which can lead to malnutrition and famine.
An epidemiologist, Slutkin has applied the tools and lessons of disease prevention to violence across the U.S. and in other countries. The End of Violence: Eliminating the World’s Deadliest Epidemic (Little, Brown and Company) sums up his insights and experiences over several decades, particularly in Chicago, Illinois, including his key insight that violence is contagious. He writes: “Violence is often regarded as an unavoidable fact of life… [but it] enters the brain and infects people, communities, and countries via the same process as other epidemics.”
Over several decades of pioneering fieldwork, Slutkin observed that violence is not primarily a moral failing, or a political inevitability arising from poverty, or about failures of policing. 
Instead, violence is a contagious, communicable disease that alters human brain biology, spreads by person-to-person transmission, and can be contained using the standard public health epidemic playbook that he had previously used to fight TB, AIDS, and other diseases. He notes the threat of super-spreaders, such as authoritarian leaders who abuse their platforms to mass-infect populations with violent ideologies or behaviors.
Slutkin finds that transmission is “dose dependent:” “Children who were exposed to intermediate or high levels of violence, especially those who experienced chronic exposure, were over 3,000 percent or 31.5 times more likely to engage in chronic violent behavior than those who were exposed to no or low amounts of violence.”
Violence not only directly hurts people; it has indirect harms. For example, when there is violence in communities, it prevents student learning and discourages teachers.
“We already have the tools to protect ourselves, heal our communities, and end violence in our lifetime. It is now up to us to use them.”
He argues that the cutting edge of public health is prevention via interaction with people to move them away from heighted risks.
Slutkin’s program trains “violence interrupters” and credible messengers (often individuals who have transformed their own lives after involvement in street violence) to identify and mediate conflicts before they turn lethal (the rough health equivalent of contact tracing and quarantine).
“To interrupt the transmission… we need to follow a new playbook, one grounded in public health… our most formidable tool to limit spreading is helping a population adopt safer behaviors… There is no epidemic control without changes in behavior.”
Dr. Ron Waldman, who worked with him in Somalia, writes: “Slutkin has taken incredibly innovative thinking, adapted from his experiences in global health, and applied it with remarkable dedication and even more remarkable results, to one of the most enduring and destructive social problems plaguing the U.S. This is an important book.”
His program, formerly called Ceasefire, now “Cure Violence Global” (CVG), has been replicated in hundreds of communities across 17 countries, and major cities in the United States. These includes:
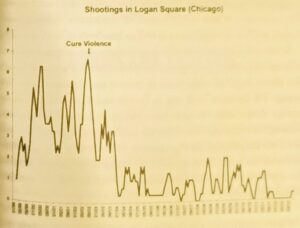
- * West Garfield Park, Chicago, where deaths dropped by 31.4% in the first year;
- * San Pedro Sula, Honduras, where shootings declined by 94%;
- * South Bronx, East New York, Brooklyn;
- * Port of Spain / Trinidad and Tobago; and
- * Cali, Colombia, where 30-50% of homicides were reduced.
Dr. Manuel Carballo, who has worked with him for many years, says: “Dr Gary Slutkin’s work to prevent violence has not only reminded us of the magnitude of this global problem, but more importantly has explored the complex of factors that contribute to what he has so rightly and innovatively defined as a communicable disease. His work and his book is a game changer. It reflects a social tragedy that is all too often taken for granted or that generates responses that simply skim over the insidious character of the problem. The insights he provides should now serve as a guide for policy makers and the public at large, and hopefully will lead to new and concerted action. Dr Slutkin has pioneered a whole new public health arena and has been able to demonstrate that the incidence of violent behaviour can be effectively reduced. The implications of this for public health and human security are far-reaching.”
CVG is a nonprofit that provides training, technical assistance, assessment, capacity building, hiring support, monitoring, and ongoing guidance rather than directly running every local program. Local community-based organizations or governments usually implement the on-the-ground work (violence interrupters, outreach workers, etc.).
Slutkin writes, “We needed locals who had firsthand experience with violence. …This was equally true in the epidemic work I did… If we wanted to reach Somali refugees, we needed to hire other Somali refugees. If [we] wanted to help change behavior among intravenous drug users, [we] needed to hire former intravenous drug users. People trust people they recognize themselves in, and, ideally, already know.”
In his concluding Action Plan, he recommends: “Every city and community needs a violence-prevenion program, just as it needs police departments, fire departments, schools and health services.”
The books end-notes and “Solutions by Violence Syndrome Annex alone are worth the price of the book’s purchase.
The dominant funding source for CVG has been municipal and state government budgets, increasingly treating the program as recurring line items rather than one-off grants. Baltimore’s Safe Streets, for instance, became part of the city’s budget; NYC’s tens of millions flow through the city’s Crisis Management System; St. Louis committed multi-year city money through its Board of Aldermen.
 Local health departments frequently act as the fiscal intermediary. Private donors also make a difference, such as Bader Philanthropies, which gave $100,000 to the City of Milwaukee to implement Ceasefire. Other funders are the Robert Wood Johnson Foundation, and the MacArthur Foundation. International work has involved the World Bank and Inter-American Development Bank.
Local health departments frequently act as the fiscal intermediary. Private donors also make a difference, such as Bader Philanthropies, which gave $100,000 to the City of Milwaukee to implement Ceasefire. Other funders are the Robert Wood Johnson Foundation, and the MacArthur Foundation. International work has involved the World Bank and Inter-American Development Bank.
Over the years, institutions like the Department of Justice, Johns Hopkins University, and the Centers for Disease Control and Prevention (CDC) have evaluated these interventions, frequently validating significant statistical associations between Cure Violence implementation and reduced violence rates.
The program is cost-efficient. Costs of implementation have varied from site to site, from $80,000 for a one-year startup, to $64 million in New York City. Societal savings of CVG are often estimated at $7–$33+ per $1 invested due to reduced medical, criminal justice, and other costs.
The strongest evidence comes from quasi-experimental evaluations: difference-in-differences, synthetic controls, interrupted time series, comparison neighborhoods, before/after analyses, and mixed-methods evaluations. The 2025 systematic review identified 13 papers, covering 27 program sites and 83 findings on shootings or killings. Overall, two thirds of findings showed reductions. Outside Baltimore, 95.8% of sites showed reductions and 54.2% reached statistical significance. Hunger Notes generated CVG’s Theory of Change diagram, shown here.
While the CVG has been effective at local gun violence at the community level the evidence is less compelling for larger systematic political violence, state violence, civil war, and international war.
The Nobel Peace Prize committee should consider Slutkin for candidacy.
See also: TED Talk “Let’s treat violence like a contagious disease”
See: GarySlutkin.com
https://www.youtube.com/watch?v=AWjq0tlq1bs
PBS/Frontline produced a documentary about “The Interruptors”, available here.


 courage and flexibility in his work. Always highly intelligent… loved field work. He always had a jovial spirit and a twinkle in his eye.”
courage and flexibility in his work. Always highly intelligent… loved field work. He always had a jovial spirit and a twinkle in his eye.”